The Healthcare Coalition Response Team (HCRT) conducts the response activities for the Coalition and provides a more robust operational capability than the Duty Officer and Notification Center Technician functions alone. The HCRT accomplishes the Coalition’s response objectives (see Section 2.1.2) during an emergency.
2.3.1 Composition of the HCRT
The HCRT is composed of personnel from Coalition member organizations who perform the key response functions of the Coalition, and an organizational liaison from each Coalition member to directly represent the healthcare organization. It is important to recognize that the staffing arrangement for the HCRT will vary based on the complexity of the Coalition and the needs of a specific incident. In many situations, the HCRT functions can be performed by a minimal number of staff.
2.3.2 Scope of HCRT Activities
The scope of response activities performed by the HCRT will vary from one Coalition to another depending on the response objectives established during Coalition development (see Chapters 5 and 6). The HCRT’s activities do not inhibit any individual organization’s response and recovery actions. The responding organizations conduct whatever actions they need to during an emergency, but they share information and develop common efforts where indicated and advantageous to the Coalition members. Similarly, the Coalition does not supplant the local public health agency’s response activities.
2.3.3 Recommended Management Strategy for the HCRT
NIMS does not specify any one structure for managing MAC System activities. Emergency Management Institute (FEMA) training (IS 701) presents several models that have been used by government agencies for establishing and managing EOCs. These models may be examined for relevance in managing the HCRT.[6]
The authors of this handbook recommend an ICS-based model for managing the HCRT because this approach has been validated in managing many types of com plex activities under emergency conditions. It is important to understand that using ICS in a MAC System does not mean that the EOC-like function (i.e., the HCRT) is managing the incident itself. The HCRT supports the incident managers, whether the incident is based at the jurisdictional level (Tier 3) or a member organization (Tier 1). Using an ICS-based structure also ensures consistency with NIMS and with the organizing strategy used by most healthcare organizations for their own EOPs. The Hospital Incident Command System (HICS), which has been adopted by many healthcare organizations for incident response, is based on ICS.[7]
While the ICS-based model employs the traditional IMT structure (Figure 2-2), the responsibilities and processes addressed in the HCRT may be somewhat simplified. For example, because the Administration/ Finance Section may have minimal responsibility in a Healthcare Coalition response, it may be subsumed as a supporting function within the Planning or Logistics Sections (this is consistent with NIMS guidance).
|
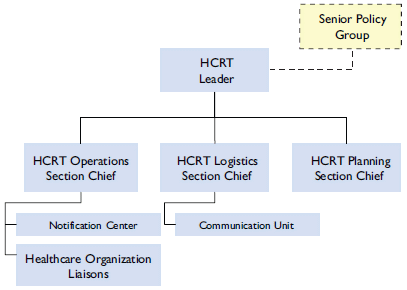
Figure 2-2. Basic configuration for the HCRT
|
| Figure 2-2: An HCRT Leader, who will report to the senior policy group, oversees the HCRT Operations Section Chief, HCRT Logistics Chief, and HCRT Planning Section Chief. The HCRT Logistics Section Chief works with a communication unit and the whole system will receive input from the notification center. Healthcare Organization Liaisons are crucial for providing feedback and information. |
|
|
As with traditional ICS descriptions, only the HCRT positions that are required to respond to an incident are activated. The size and complexity of the HCRT may vary significantly in each locale. In fact, it is expected that most Healthcare Coalitions will respond to a majority of incidents with one to three individuals conducting all HCRT functions. Conversely, complex Coalitions or those responding to very complex incidents could require a more robust response organization. The key functions of the HCRT are outlined below for consideration.
Leader (equivalent to Command in traditional ICS)
This function oversees all HCRT activities. Because there is no inherent “command” authority within the Healthcare Coalition and the Coalition does not directly manage the incident, the term “Leader” is more appropriate to describe this function within the HCRT. Since this function is responsible for all HCRT activities, it is the one function that must always be staffed for any incident.
Operations Section
Depending on a Coalition’s response objectives, the Operations Section of the HCRT would be responsible for several activities. If response activities are particularly complex for an incident, this Section may be subdivided into branches, divisions, or groups, but this usually will not be necessary. Factors that may influence the branch construct include the number and size of the organizations within the Coalition, and the complexity of the data and information being processed.[8] Example activities for the HCRT Operations Section include:
Information management: Provide an information “clearinghouse” to promote enhanced situational awareness. The term clearinghouse is used to emphasize that information is collected, aggregated, and transmitted to healthcare organizations with only transparent processing of the data. All member organizations are treated equally and provided with a common operating picture of the incident. This promotes consistency in decision-making across the organizations.
Resource coordination and support: Facilitate the ability of member organizations to obtain resource support under the time urgency, uncertainty, and logistical constraints of emergency response. It does not preclude the use of day-to-day resource acquisition methods, nor does it supplant the importance of developing resource acquisition and management methods at each healthcare organization (Tier 1). Rather, it provides a platform for disseminating resource requests from impacted organizations. In addition, the HCRT may facilitate communications between requesting organizations and those willing to provide resource support.
Response coordination: Promote comprehensive and consistent incident action planning by Coalition member organizations through the sharing of response objectives, strategy, and major tactics. Task forces may be established to address unusual response issues, such as urgently needed, consensus-based diagnostic or treatment guidelines, patient transfer protocols, tracking of evaluated patients, or other actions.
Community response integration: Facilitate the integration of the healthcare response into the general community response by promoting exchange of information between member organizations and responding Jurisdictional Agencies (Tier 3).
During response, the HCRT Operations Section interfaces with the member organizations through their designated HCRT Organizational Liaison within the member organization’s IMT.[9] This liaison position must be established to ensure efficient Coalition response activities. Depending upon how the Coalition is constructed, the Organizational Liaison could be responsible for:
- Receiving information from the HCRT and acknowledging receipt of the information
- Transmitting information from the HCRT to decision makers within the organization (e.g., the organization’s IMT)
- Supervising the response to requests for information or resource assistance that comes through the HCRT
- Participating in meetings or teleconferences convened by the HCRT to bring together healthcare organizations.
Support Functions
Consistent with the ICS model, the HCRT may wish to develop the following Sections to support its response operations. Even if a Coalition defines specific positions for HCRT response functions, it is important to recognize that the positions are only staffed as needed. Position descriptions should be developed, and training and exercises conducted, to develop the knowledge, skills, and abilities for staff.
Planning Section: Depending upon the complexity of the Healthcare Coalition, the Planning Section could perform a number of response activities focused on aggregating incoming data and formatting information reports to return to member organizations. This collated information is usually conveyed to jurisdictional authorities (Tier 3). The following responsibilities for the Planning Section are presented for consideration:
- Aggregate, analyze, format, and document relevant incident information in standard reports. For example, the Planning Section may document incident details or the resource status of member organizations, such as available patient beds.[10] The data should be captured in a standardized format and provided to all Coalition member organizations and relevant Jurisdictional Agency(s) (Tier 3).
- Facilitate internal HCRT meetings. The Planning Section can facilitate meetings or teleconferences for internal HCRT planning. For meetings involving Coalition member organizations (Tier 1), it may be more appropriate for the HCRT Operations Section to facilitate, since these discussions support achievement of the HCRT response objectives. The purpose, format, and ground rules for each type of meeting should be pre-determined.
- Oversee action planning for the HCRT: In robust Coalitions, the HCRT may wish to conduct formal action planning when indicated by incident circumstances. Action planning is well accepted in MAC Systems even though these systems do not command an incident. The Planning Section could be tasked with assembling and completing the action plan for the Healthcare Coalition. If created, the HCRT action plan should be shared with Coalition member organizations and jurisdictional authorities. The plan itself may be shared or it may be discussed in an operations briefing (often conducted virtually) with relevant organizations.
Logistics Section: Per ICS principles, this Section provides logistical support to the HCRT and is distinguished from support that is provided to Coalition members, which is a function of the HCRT Operations Section. Because many of the HCRT’s activities during emergency response and recovery can be conducted virtually, the key logistical issue will be supporting the information and communications technology that is used by the HCRT and its member organizations. For example, the Logistics Section may address a Coalition member organization’s difficulty accessing web-based programs or troubleshoot issues with radio equipment. Other types of support that may be performed by the Logistics Section include:
- Staff scheduling for HCRT positions during prolonged incidents
- Resource support to the HCRT and the Coalition’s Notification Center, including facilities, transportation, and other resources
- Services support, such as food and drinks, communications and information technology support, sleeping quarters, etc.
Administration/Finance Section: Per ICS, this Section focuses on administrative and finance support to the HCRT and is staffed only as needed. This becomes important if there is an expectation for reimbursement for some of the distributed HCRT activities, such as reimbursing member organizations for employee time devoted to HCRT positions staffed during an emergency. Other cost tracking may include any expenses assumed by an organization that provides a physical location for HCRT operations or the Coalition Notification Center. This Section notes when spending may be approaching limits set by the Coalition Senior Policy Group and brings this to the attention of the HCRT Leader. This function is expected to be rarely staffed as a separate HCRT Section.
2.3.4 HCRT Requirements
In order for the HCRT to function as intended, the following requirements must be met:
- Communications and information technology must be available 24/7 for use by the Healthcare Coalition. This may include a messaging system (text and/or voice), a radio system, relatively secure teleconferencing methods, satellite phones, Voice Over Internet Protocol (VoIP), and technology to support web-based interaction between Coalition member organizations and between the Coalition and jurisdictional authorities (Tier 3). A good cost-saving measure is to use technologies established for other purposes (e.g., using a webbased system established for a Jurisdictional Agency). However, it is important that the technology is always available for dedicated use by the HCRT during emergency response.
- Personnel must be identified to staff the HCRT during incident response. These individuals will usually be employees of the Coalition’s member organizations. Because these organizations may be impacted by a hazard, candidates for the HCRT should be identified from as many organizations as possible and focus should be on streamlining the staffing of the HCRT during emergency response and recovery.
- Procedures should be established to maintain HCRT activities despite a hazard impact, with backup resources identified for each essential HCRT function.
Exhibit 2-1 highlights some of these requirements as applied to a Healthcare Coalition in Minnesota.
Exhibit 2-1: Regional Hospital Resource Center (RHRC) in the State of Minnesota
The State of Minnesota has been divided into eight regions, each having developed a response organization that coordinates the efforts of healthcare assets within its respective geographic region. Though the regions align with Public Health and Emergency Medical Services (EMS) regions within the State, they do differ from State Patrol and Homeland Security and Emergency Management (HSEM) regions.
Each Healthcare Coalition spans multiple independent jurisdictions and coordinates response information among its participating healthcare organizations, including hospitals, healthcare systems, and clinics (clinic coordination is less formal at present and variable between regions). This requires direct communications with each individual jurisdiction covered by the Coalition when coordinating healthcare assets during incident response. This important activity ensures a common operating picture for all local authorities.
The Healthcare Coalition that includes Minneapolis is based at Hennepin County Medical Center. Its day-to-day communications center is utilized to coordinate healthcare assets located within this response Coalition. Communications to individual healthcare assets are based on internet, 800 MHz radio, and telephonic communications. A Duty Officer is always available to receive notifications and this contact method is disseminated to public safety agencies. If the Healthcare Coalition response organization is to be activated, the staffing typically involves 3-4 personnel to cover all the functions of the response organization. These personnel are “donated” by individual healthcare organizations and may be supplemented by staffing from the local Medical Reserve Corps (MRC).
The response activities can be conducted from the communications center or in a more distributed fashion (personnel remain at their location of regular employment). In addition, Coalition personnel have the capability to deploy to the Emergency Operations Center (EOC) where they can more directly interface with Public Health, Emergency Management, and EMS. The Coalition has the capability of convening regular teleconferences as required for its participating organizations.
After the Interstate 35W Bridge collapse in Minneapolis on August 1, 2007, the RHRC assisted EMS with organizing patient lists, tracking delayed casualties, and providing Family Support Center staff and support. The RHRC also coordinated with Minnesota Department of Health and other agencies to provide awareness of available healthcare assets.
- FEMA Emergency Management Institute, IS 701, NIMS Multiagency Coordination System. Accessed May 7, 2009 at: http://training.fema.gov/EMIWeb/IS/is701.asp.
- State of California Emergency Medical Services Authority, Hospital Incident Command System Guidebook, (August 2006); Available at: http://www.emsa.ca.gov/hics/default.asp.
- The organization of Operations Section branches is further discussed in Chapters 3 and 4.
- Another title, such as Point of Contact or “POC,” may be used for this staffed position at each Healthcare Coalition member organization.
- The actual collection of data and dissemination to individual healthcare organizations (Tier 1) and jurisdictional authorities (Tier 3) is an Operations Section function. The actual collection of data and dissemination to individual healthcare organizations (Tier 1) and jurisdictional authorities (Tier 3) is an Operations Section function.
<<Previous - Return to Top - Next>>

